
Whether you get an epidural or not is a personal decision. Every person’s birth experience is different and some may have a different vision for their labor process.
Labor epidurals are very common. A study done by Stanford University showed that nearly 71% of pregnant patients in the United States opted for an epidural birth.
There is a lot of misinformation surrounding labor epidurals, so I’m here to clear the air. As a labor and delivery nurse, I have participated in many epidural placements and have learned tons from anesthesiologists.
Disclaimer: The information in this post is purely for entertainment and is not meant to replace the advice of a medical professional. This is not medical advice.
What is a labor epidural?
Epidural analgesia is a fancy way to say “pain relief from an epidural block.”
Placed by an anesthesiologist or a nurse anesthetist, an epidural is a small catheter, or thin tube, that is placed through the lower back into the epidural space of your back. Then, a small amount of medication is administered through that tube to block pain signals to your lower body. You are typically numb from the bottom of your ribcage down to your toes.
Epidurals are great for relieving contraction pain, but they typically do not get rid of the pressure. Most pregnant patients are able to feel pressure as the baby’s head as it enters the birth canal. This pressure helps guide pushing and is a great sign of labor progress. Most people describe it as feeling like they need to poop.
So while you may be uncomfortable towards the end of labor with an epidural, it definitely helps by eliminating contraction pain.
What’s the difference between an epidural block and a spinal block?
An epidural block is different from a spinal block. With a spinal block, medication is injected into the dura mater to numb the spinal nerves. You are instantly numb and unable to move the lower part of your body.
With an epidural, it takes longer to feel pain relief (about 15-30 minutes) and you’ll likely feel slight pressure sensation and have some mobility. Some patients with an epidural are able to independently change positions within the bed.
Spinal blocks are most often used for cesarean section. This allows you to be awake and alert during your baby’s birth. Typically you are only put to sleep under general anesthesia for a c-section if it is an emergency situation.
An additional bonus of having an epidural placed is that it can be used to numb you for a c-section if necessary. Your anesthesia team can give you a big dose of numbing medication if you needed a cesarean delivery.
How epidurals are done step by step
If an epidural is part of your birth plan, you’re probably wondering how it’s going to happen. This is the process for getting your epidural anesthesia set up.
WARNING: Graphic images ahead.
Step one: consent and preparation
After you request an epidural, the anesthesiologist or nurse anesthetist will come and introduce themselves. They will discuss all of the benefits and risks to you, and at the end they will ask if you would still like an epidural. They will do a thorough exam and as about your health history to make sure an epidural is a good fit for you.
Your nurse may give you a few bags of IV fluids before the epidural placement. This is because one of the possible side effects of epidural medications is low blood pressure. Changes in blood pressure affect the blood flow to baby through the placenta. Giving IV fluids helps to prevent this from happening.
Certain medical conditions may make you more likely to experience this.Your healthcare provider can give you additional medication to improve your blood pressure if it were to drop.

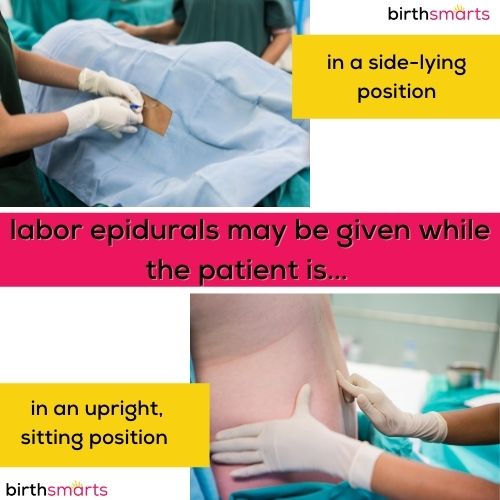
Step two: finding the right position
The anesthesia team and your nurse will help you get into the right position for your epidural. This is usually sitting or lying on the side of the bed with the anesthesiologist behind you.
Step three: cleaning and prepping the area
Once you are positioned, they will clean your back off with soap. Next, you’ll feel the anesthesiologist pushing around on your back between your vertebrae. He/she is trying to find the perfect spot to place your epidural so that you are numb in all the right areas.

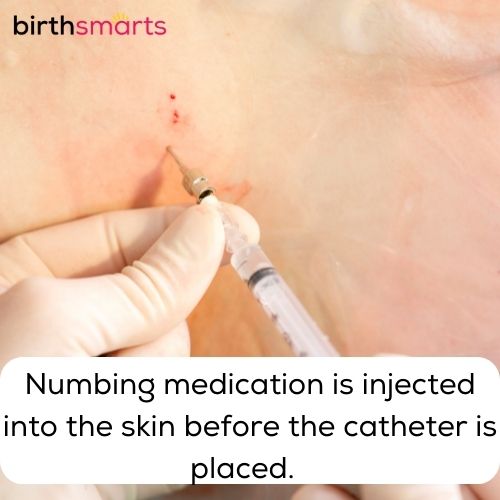
Step four: numbing medicine
When the anesthesiologist finds the spot to place the epidural, they will inject some numbing medicine called local anesthetic. This is the only part of the epidural placement that should hurt! Most people describe it as a bee sting or burning sensation that quickly subsides.
The local anesthesia feels like a quick sting. A few seconds after the numbing medicine is injected, that area of your back should be numb. All you should feel is the pressure as they place the epidural needle. This pressure feels like they are pushing on your back with a finger.
Step five: placing the catheter
The anesthesiologist will then place a needle between the vertebrae into the epidural space of your back. The epidural space is the space between your vertebrae and your spinal cord.
Once they are in the right spot, they will thread a small catheter through that needle. The epidural catheter is about as thick as fishing wire, and is a very small, thin and flexible tube.
Then, the needle is removed, and the catheter stays in place. They will put lots of tape on your back to hold the catheter in place.

Step six: testing the placement
Next, the anesthesia team will administer a “test dose” to make sure the catheter is in the perfect spot. They will monitor your heart rate and oxygen while injecting a small amount of medicine through the catheter.
If you notice any unusual symptoms, it is important to speak up. That could mean the epidural is not in the proper spot and will not work. If that happens, they may readjust the catheter and try again. If you do not experience any weird sensations, they will start giving you the epidural medication.
Step seven: getting some relief!
Once the catheter is taped on your back and secure, they may give you a bolus dose, or a small boost of medication to help you feel comfortable quicker. Then they will hook the epidural up to a pump and give you a continuous infusion of medication to keep you comfortable.
The entire process of placing the epidural takes between 15-30 minutes.
Typically, you start to feel relief within 20 minutes of the bolus dose. Most people report contractions feeling shorter and shorter until they do not notice them anymore. The goal is that you should be comfortable until you start feeling the rectal pressure from the baby’s head moving lower and lower into the birth canal.

After you get your epidural, you won’t be able to tell when you need to use the bathroom. Your nurse will place urinary catheter to help drain your bladder. This is usually removed once you are pushing.
How long does an epidural last?
Once you are comfortable and no longer feeling much pain, your epidural medication will be continuously given to you in a low dose.
Pain relief from an epidural should last until after the baby is born. Once the baby is born, the medication pump will be turned off. You are typically able to get up and move around within 2 hours of the medication being off.
Sometimes people with an epidural feel some labour pain return. If this happens, it is important to let your care team know right away! Additional medication can be given to keep you comfortable or your care team may give you a button to push to give yourself a boost of medication. Don’t worry – you can’t overdose yourself. The machine is programmed to only give a set amount.

How quickly do epidurals work?
Unfortunately, epidurals aren’t instant pain relief. But the good news is you should feel less pain within 15-30 minutes.
How will I know when to push with an epidural?
Most people feel rectal pressure when it is time to push. People often explain it as the feeling like they have to have a bowel movement. This is because baby’s head is pushing against the rectal nerves.
The pressure will start off being intermittent and only with contractions and eventually will become constant. This is usually a great sign that you are almost ready to start pushing and the baby’s head is moving lower and lower into the birth canal.
While this pressure is very uncomfortable and often intense, it is usually not painful.
In rare cases, some patients don’t feel any pressure with the baby’s head. If that is the case, your nurse or provider will likely see changes in the baby’s heart rate pattern or your contraction pattern to indicate delivery is near.
Side effects from labor epidurals
There are very few epidural side effects. Most adverse effects are mild and resolve quickly.
Back pain at the injection site is very common from the epidural placement. It is usually temporary, and tends to go away hours to days after the epidural is placed. Chronic pain is a very rare side effect from epidurals.
Sometimes there is a temporary drop in blood pressure due to the epidural medication. This is usually prevented by giving a bolus dose of IV fluids before getting an epidural, and it can be easily treated with IV medications if necessary. This side effect is usually seen in the first 30 minutes of getting an epidural.
Rarely, a complication called a spinal headache occurs. This is a severe headache that happens when there is a leakage of spinal fluid where the needle has punctured. A spinal headache is treated with something called a blood patch and is most likely to occur a day or so after the epidural is placed. This kind of headache is different from a normal bad headache as it typically resolves when you are lying flat.
Of course, any time there is breaking of the skin there is a chance for an infection. Because of the cleaning and sterilizing of the lower back before the epidural is placed, the risk of infection is very low.
Long term side effects from epidurals are extremely rare. There is a very slight risk of permanent nerve damage. According to the American Society for Regional Anesthesia and Pain Medicine, the risk of nerve injury can occur anywhere from 1 in 4000 to 1 in 200,000, depending in the type of nerve block used and other specific risk factors.
After you receive an epidural, you are unable to get out of bed and move freely. This is because your legs become numb and hard to move and feel. Because of this, you are at higher risk for developing a blood clot. Your care team may recommend using compression stockings to reduce your risk.
Overall, the risk of serious complications is low with epidural use.

Who can’t have an epidural?
Epidurals aren’t for everyone. There are a few instances that would make an epidural unsafe.
Your provider will discuss with you if they feel an epidural isn’t a safe choice for you. Some instances include:
- People on blood thinners or with a very low platelet count
- Those with an allergy to the medications used in the epidural
- People with severe spinal deformities, like scoliosis or spinal stenosis
- There is no anesthesiologist on staff
- There is not enough time to receive one before the baby is born
What’s the best time to get an epidural?
In my opinion, the best time to get an epidural is when you feel your contractions are becoming unbearable. I usually recommend my patients have 3-4 consecutive contractions that feel very intense before requesting one.
Ideally, you would get an epidural once you are in active labor. Labor should be moving along and the baby should arrive within a few hours.
This is not a firm rule. Patients are always in control and can request an epidural any time. Some patients may want an epidural in early labor – especially if they are having a lot of back labor or are becoming exhausted and having difficulty resting.
When is it too late to get an epidural?
Every facility has different protocols regarding when it is too late to get an epidural. Most places do not have a set time or dilation where you are too late for an epidural as long as you can sit still in the right position.
Your team needs to be confident that the baby is not going to be coming within the hour before they can place an epidural. Remember, it may take 15 minutes for you to get your IV fluids, another 20 minutes to place the epidural, and another 20 minutes for the epidural to start working! You need at least 1 hour before birth to get an epidural.
You also need to be able to sit still for the epidural. This reduces your risk for things like nerve damage.
Other pain management options
While epidurals are a great way to relieve pain in labor, there are many other ways to relieve pain as well!
Ask your care team about what other options you have for pain relief. Here are some common options:
- Nitrous oxide: a gas that you inhale to reduce anxiety and pain. This requires active effort and makes it difficult to rest.
- IV pain medications: These medications work quickly to reduce pain, but can make you feel weird or loopy. They typically only last a few hours at a time.
- Morphine: given as an injection, this medication is usually given in early labor. It’s great for taking the edge off of contraction pains and is a good thing to try if you need some rest.
- Other pain relief options: breathing techniques, movement and position changes, using heat/ice and soaking in a tub are also great ways to reduce pain.
Is a labor epidural on your birth plan? Why or why not?